One of the fundamental pillars of the fight against tuberculosis
(TB) is addressing the family and social environment of each
patient. Each bacilliferous patient may infect about 20 individuals,
especially when they live close to each other. Of the infected
individuals, a non-negligible percentage (5 to 10%) will develop
tuberculosis disease.
For intervention purposes, an outbreak is considered to be the
occurrence of one or more cases of TB originating from the same
index case within one year after the diagnosis of the primary case.
When case clusters have been established using molecular techniques,
clustering is defined as the detection of two or more cases of TB
with identical RFLP-IS6110 patterns, or, in strains
with less than six bands of the RFLP-IS6110
pattern, the strains that share the same spoligotyping, PGRS-RFLP,
or MIRU-VNTR patterns
(Centro Nacional de Epidemiología. Instituto de Salud Carlos III. Red Nacional de Vigilancia Epidemiológica, 2013).
The occurrence of an outbreak may be favoured by various factors
such as the following:
The detection of TB outbreaks is one of the main activities for
the control of this disease. The study of outbreaks provides
information about the transmission and the environment where the
disease occurs.
The objectives of contact investigation are to successfully
interrupt the chain of transmission of TB and to prevent future
cases and disease outbreaks from occurring. It is also important to
note that all TB cases begin as a TB contact.
CONTACT INVESTIGATION METHODOLOGY
All healthcare workers taking care of TB patients should make
sure that the individuals who have been in close contact with
patients with potentially communicable TB are assessed and treated
in accordance with international recommendations.
Whenever possible, the chain of transmission should be re-created
to identify the initial case (especially in children under 15 years
of age). This will be done by following the concentric circle
approach
(Figure 1. Classification of contacts according to the
concentric circle approach)
(Table 1. Figure 1. Classification of
contacts according to the concentric circle approach Transaltion)
, which classifies contacts into high, medium, and low risk:
-
High risk of infection (high-risk contact, close contact):
bacilliferous index case and/or exposure to an environment
favourable to transmission for at least 6 hours a day, or for a
shorter period of time if the contact’s immune system is
compromised, if the individual is under 5 years of age, or if
the source of infection is part of a micro-epidemic. This
includes cohabiting contacts, non-cohabiting contacts (children
sharing the same classroom or premises, school, kindergarten,
nursery school, and other educational or social centres, and
circle of close friends), and contacts in closed groups.
-
Medium risk of infection (frequent contact): exposure to an
environment favourable to transmission for less than 6 hours a
day, without the conditions mentioned in the previous point.
-
Low risk of infection (sporadic contact): when the risk of
infection is similar to that of the general population.
Non-daily contact.
Figure 1. Classification of contacts according to the
concentric circle approach
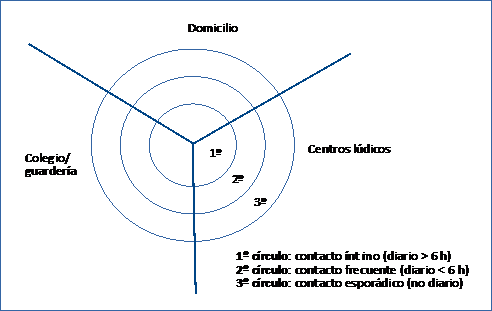
Source: Adapted from: Documento de consenso sobre el
estudo de contactos en los pacientes tuberculosos
(Alcaide et al., 1999).
Table 1. Figure 1. Classification of contacts according to the
concentric circle approach Transaltion
|
Spanish
|
English
|
| Domicilio |
Home |
| Colegio/guardería |
School/Nursery |
| Centros lúdicos |
Leisure centres |
| 1º circulo: contacto íntimo (diario > 6 h) |
1st circle: close contact (daily > 6 h) |
| 2º circulo: contacto frecuente (diario < 6 h) |
2nd circle: frequent contact (daily < 6 h) |
| 3º circulo: contacto esporádico (no diario) |
3rd circle: sporadic contact (not daily) |
According to this model, the study should be initiated by
investigating the contacts who are most at risk (the first circle),
and then be extended until the prevalence of infection found is as
expected in that population. If a new bacilliferous case is detected
among the contacts, the concentric circle approach must be initiated
once again starting from this case.
The urgency of the initiation of a CI and its extent should be
based on the likelihood of transmission of the infection and its
possible consequences, especially in children and immunosuppressed
contacts, whose risk of becoming ill after infection is higher (Table 2. Risk of TB after infection in immunocompetent
children).
Table 2. Risk of TB after infection in immunocompetent
children
|
Age at Mycobacterium tuberculosis
infection
|
Risk of pulmonary disease or mediastinal
lymphadenopathy (%)
|
Risk of meningeal or disseminated tuberculosis
(%)
|
| < 12 months of age |
30-40 |
10-20 |
| 12-24 months of age |
10-20 |
2-5 |
| 2-4 years of age |
5 |
0.5 |
| 5-10 years of age |
2 |
< 0.5 |
| > 10 years of age |
10-20 |
< 0.5 |
1. CI phases and action guidelines
Determining the time period in which the index case might
have become a source of infection is important and may be
achieved by conducting a survey. However, when this is not
possible, the following are accepted:
-
Three months prior to diagnosis when the index case is
bacilliferous and/or presents with cavitations in
radiological images.
-
One month prior to diagnosis when the index case is not
bacilliferous.
-
Three months prior to diagnosis in HIV-immunosuppressed
patients, often with atypical chest X-rays that can delay
diagnosis and increase the transmission period.
-
Preparation of the contact census.
-
Prioritisation and classification.
-
Tuberculin test (TT)/ interferon gamma release assay test
(IGRA): In the context of a CI, indurations of ≥ 5 mm in
children, HIV-positive individuals, immunosuppressed
individuals, close contacts of bacilliferous patients, and
individuals with x-ray lesions suggestive of previous
untreated TB are considered to be positive (whether or not
they have been BCG-vaccinated).
-
Chest X-rays of the selected positives and contacts (see
below), to rule out disease.
-
Diagnosis and contact management.
Depending on the results, the contacts are classified as
follows:
-
Not infected: chemoprophylaxis (CP) should be considered
following the criteria set out in the article ADDRESSING
TUBERCULOSIS IN CHILDREN (exposed child). The test should be
repeated at 8-12 weeks in high and medium priority
contacts.
-
Infected, but not diseased: treatment of TB infection (TTI)
should be considered following the criteria set out in the
article ADDRESSING TUBERCULOSIS IN CHILDREN (infected
child).
-
Diseased individuals: their treatment is established and
the investigation of their contacts is organised.
-
Treatment supervision and follow-up.
-
Expanding the CI, if necessary.
-
Recruitment of contacts who had not been investigated
previously and individuals who failed to comply with the
treatment.
-
Closure and final assessment.
The complete case history of each contact must be prepared,
placing special emphasis on the presence of symptoms consistent
with TB, history of TB disease, BCG vaccination, previous TTs,
history of preventive treatment, and the presence of risk factors.
The following situations may arise:
Both TT and IGRA techniques can be used in CIs
(World Health Organization, 2018).
,and if they need to be repeated, it is
advisable to perform the same test as the initial one. These tests
are only indicated for diagnosing infection in individuals with a
high risk of developing the disease who can benefit from
preventive treatment. This treatment should be accompanied by a
follow-up plan until completion. For low-risk individuals
(sporadic contacts), these techniques are not indicated.
Figure 2. Assessment and treatment of high and medium
priority contacts
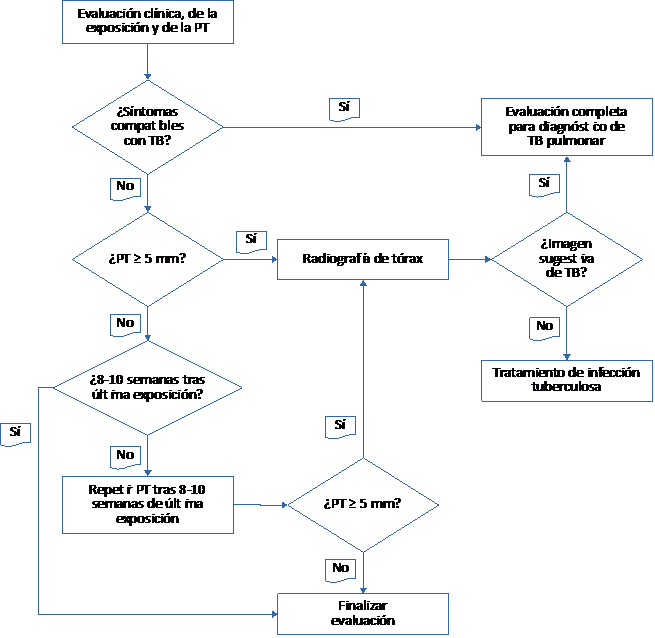
TT: tuberculine test; TB: tuberculosis
Source: adapted from: Guidelines for the investigation
of contacts of persons with infectious tuberculosis;
recommendations from The National Tuberculosis Controllers
Assotiation and CDC, and Guidelines for using the Quantiferon-TB
Gold Test for detecting Mycobacterium tuberculosis
Infection
(National Tuberculosis Controllers
Association; Center for Disease Control and Prevention,
2005).
Table 3. Figure 2. Assessment and treatment of high and medium
priority contacts Translation
|
Spanish
|
English
|
| Sí |
Yes |
| No |
No |
| Evaluación clínica de la exposición y de la PT |
Clinical assessments, exposure assessments, and TT
assessments |
| ¿Síntomas compatibles con TB? |
Are symptoms consistent with TB? |
| Evaluación completa para diagnóstico de TB pulmonar |
Complete examination for diagnosing pulmonary TB |
| ¿PT ≥ 5 mm? |
TT ≥ 5 mm? |
| Radiografía de tórax |
Chest X-ray |
| ¿Imagen sugestiva de TB? |
Does the image suggest presence of TB? |
| ¿8-10 semanas tras última exposición? |
8-10 weeks since last exposure? |
| Tratamiento de infección tuberculosa |
Treatment for TB infection |
| Repetir PT tras 8-10 semanas de última exposición |
Repeat TT at 8-10 weeks after the last exposure |
| Finalizar evaluación |
End of assessment |
2. CI in schools and nurseries
The census of contacts in schools may include a large number of
children, so communicating the actions to be carried out to staff,
parents, and the general public is important to prevent anxiety
and unnecessary media attention.
The staff that will conduct the CI must visit the centre to see
how the classrooms and interior spaces are distributed and check
ventilation and other general conditions. After-school activities
and school bus trips should also be investigated.
When the index case is a child under 5 years of age, everyone
living with them, their relatives, and close contacts should be
investigated in search of the initial case. If the initial case is
not found in this environment, the CI should be extended to the
adults in contact with them in the educational centre.
All contacts classified as high priority (close contacts) who
had not had a prior positive TT or a prior TB disease should have
a TT/IGRA at the first visit. If this is not possible, the
investigation should be carried out within one week. This period
should be less than two weeks in the case of medium priority
contacts (frequent contacts)
(National Tuberculosis Controllers Association; Center for Disease Control and Prevention, 2005).
3. TB outbreaks in children and young adolescents
An outbreak investigation involves several overlapping contact
investigations, with the resulting need for increased public
health resources.
A TB outbreak in children may indicate a possible widespread
transmission of TB. These are the main aspects to be considered in
these investigations:
-
Children should be prioritised according to their degree of
exposure (the number of hours in the same classroom per
week).
-
Properly communicating with and informing staff, parents,
and the general public, as well as to the media, is
essential.
-
When the index case is a student and the source of
infection is unknown, further investigation is needed to find
the initial case.
-
When the index case is a teacher, the children in his or
her classroom and other staff with whom he or she has had
contact with will be examined.
-
In any case, negative TTs will be repeated two months after
the last contact with the patient.
-
The need to extend the CI to other groups, such as dining
room partners, etc., may be considered.
Early diagnosis, appropriate treatment of all cases of TB
disease, and rapid identification of individuals who have been
exposed to a source of infection should be the priorities of any
TB programme in order to avoid infection or to prevent developing
the disease.
 License Creative Commons Attribution -NonCommercial-ShareAlike 4.0 International
License Creative Commons Attribution -NonCommercial-ShareAlike 4.0 International